ANTERIOR CRUCIATE LIGAMENT (ACL) INJURIES:
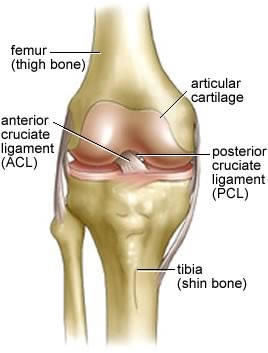
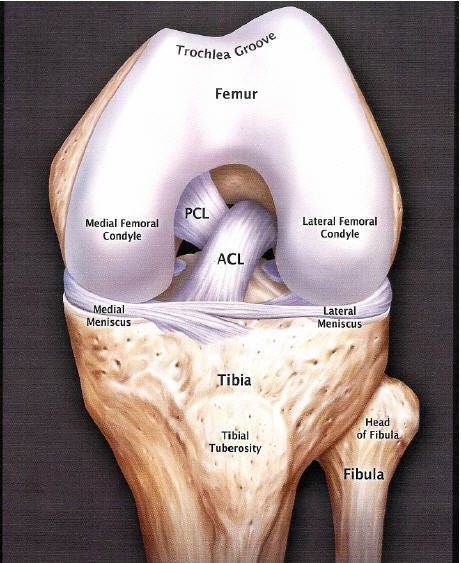
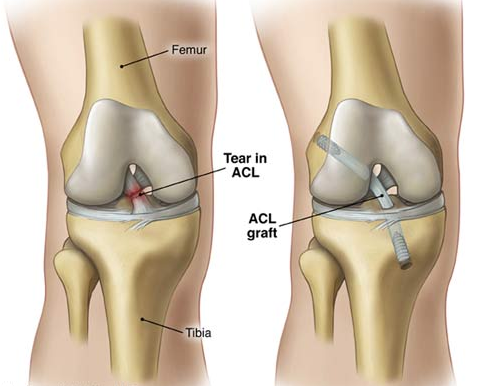
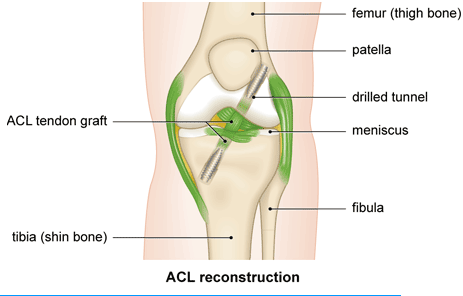
The anterior cruciate ligament (ACL) connects the tibia (shin bone) to the femur (thigh bone).
The function of the ACL is to provide stability to the knee and minimize stress across the knee joint
- It restrains excessive forward movement of the lower leg bone (the tibia) in relation to the thigh bone (the femur).
- It limits rotational movements of the knee.
There are number of nerves within the ACL which act as sensors that provide the brain with information about joint position sense (proprioception). When, for example, the ACL is stretched this information forms part of a “feedback mechanism” to activate certain protective muscle actions.
Mechanism of injury:
The ACL is particularly prone to injury during sporting activities that involve significant amounts of twisting and turning, such as skiing and football.
This injury is usually due to a sudden stop and twisting motion of the knee, or a force or “blow” to the front of the knee.
The extent of the tear can be a partial or a complete tear.
It is often injured together with other structures inside the knee joint. [Cartilage or other ligaments]
IMPACT OF ACL INJURY
- When the ACL is damaged as part of a twisting injury the patient may hear or feel a “popping” sensation.
- As the ligament has a blood supply, when torn, the knee fills with blood becoming swollen quite quickly and painful.. [Haemoarthrosis]
- Instability or a sensation the knee is “giving out” [give way/collapse ] may be a major complaint following this injury.
- Patients with injured ACL can find it very difficult to return to any sports that require twisting and turning, such as, rugby, football, squash and skiing. However, other “in line” sports such as running, cycling or cross training are often possible, despite ACL deficiency. In general, it is almost impossible to continue sporting activity after acute ACL rupture and urgent medical review is required.
SYMPTOMS:
Most patients with injured ACL have the following symptoms:
- Swelling within a few hours of the injury
- Loss of Motion [Loss of ability to extend and flex the knee]
- Distinctive “pop” heard
- “Giving-way” episodes. Your knee may collapse and you fall to the ground
- Pain with activity.
- Some people are able to continue their activity; some people’s knees collapse and they cannot walk normally
- Knee “catching” or “locking”.
DIAGNOSIS OF INJURY TO THE ACL
As with all surgical conditions, diagnosis of damage to the anterior cruciate ligament is made by a combination of:
- listening to the patient’s history
- Clinical examination
- use of modern imaging techniques e.g. MRI scan
TREATMENT OF ACL INJURIES
Treatment decisions for ACL tears are always individualized.
The decision whether to offer surgery is based on the person’s age, activity level, how unstable the knee is, and whether other structures in the knee have been injured.
Unfortunately a simple surgical repair by suturing the torn ligament together is not effective.
A successful repair involves completely replacing the torn ligaments (surgical reconstruction), and there are a number ways that this can be done.
ACL RECONSTRUCTION SURGERY
Usually surgical reconstruction is recommended to restore stability to allow people to return to desired activities and to prevent secondary damage to the menisci (cartilage cushions) and articular cartilage of the knee, hopefully avoiding premature deterioration of the knee.
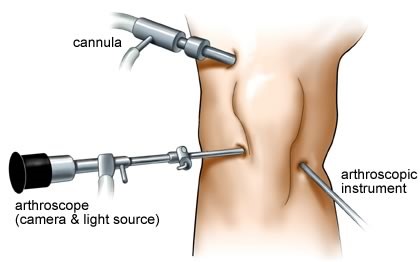
All our ACL reconstruction surgery is done arthroscopically.
We prefer reconstruction using an autograft [tissue graft harvested from the patient] rather using allograft [ cadaveric tissue] as I believe tissue from the patient results in a better reconstruction with superior long term results and lower ACL re injury rates.
Due to advances in surgical techniques, this has turned what was a major open operation to one that is now minimally invasive (via arthroscopic portals).
As indicated, there are a variety of different techniques available, but surgeons have their own preferences based on their own experience and results.
The Surgery:
ACL reconstruction involves undergoing a general anaesthetic and an in-patient stay of one night.
The operation itself lasts for just over an hour and a tourniquet is applied to the leg during the procedure.
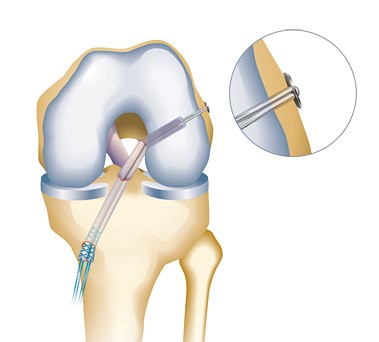
The operation is carried out under direct vision of the arthroscope (camera) inserted within the knee through key-holes.
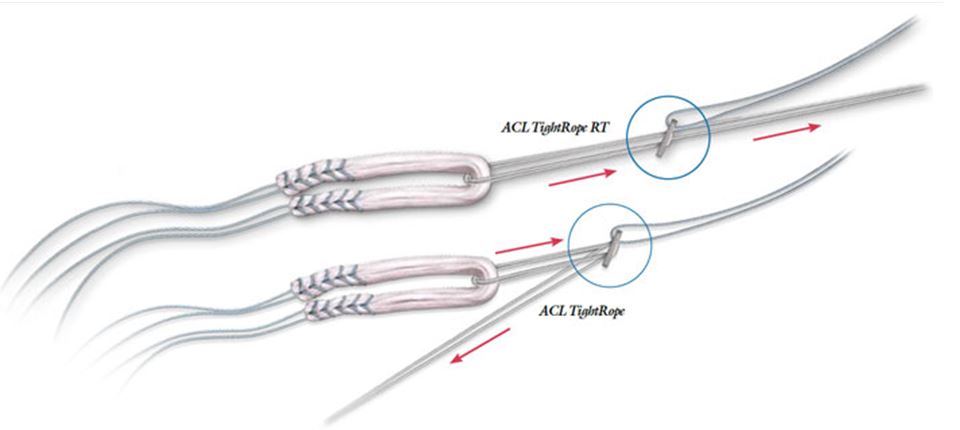
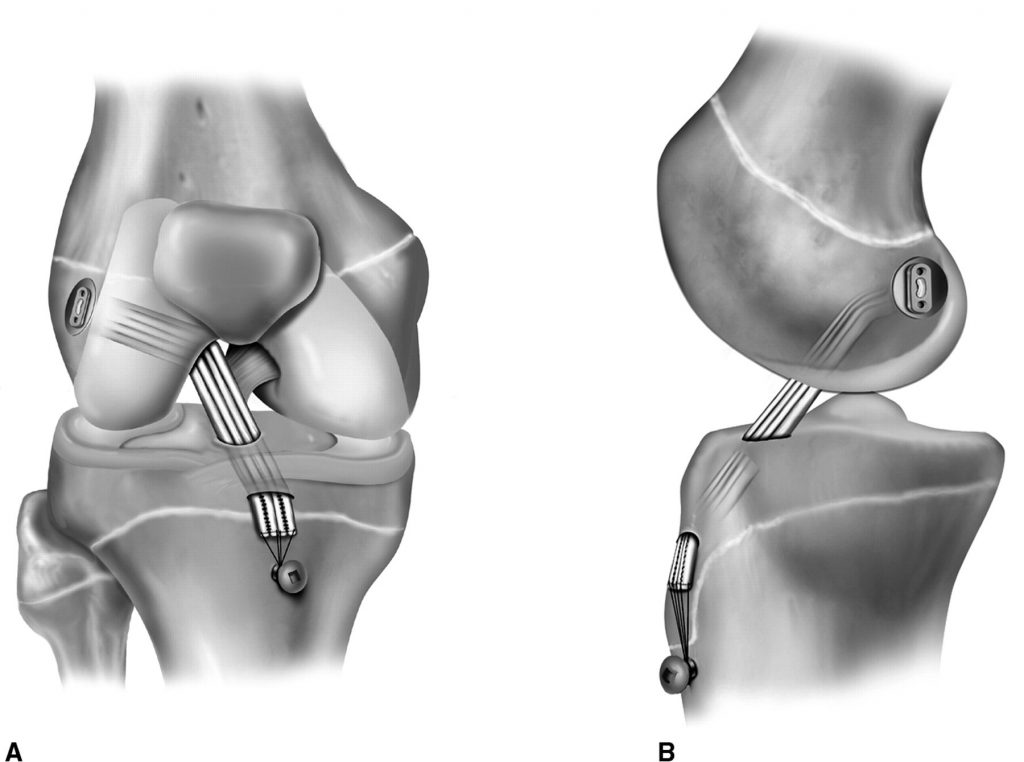
A bony tunnel is drilled within the shin bone (tibia) and the thigh bone (femur) to allow the graft to be pulled across and held in place securely.
After Surgery
Any surgical procedure has possible risks and complications. Surgeons make every effort to minimize them.
They include:
- Deep Venous Thrombosis (DVT) or Blood clots
- Infection
- Stiffness
In the immediate post-operative period, the priority is:
- muscle-strengthening
- to regain the range of motion
The post-operative programme:
- Crutches and a brace are provided for a two-week period, but you will be able to stand unsupported.
- Physiotherapy begins the day of surgery
- The sutures are removed from the wounds after two weeks
- You should be able to easily bend the knee to a right angle the day next to the surgery.
- You are expected to be able to cycle and run within three months following surgery.
- The speed of recovery from this operation is limited by the ability of the body to integrate the graft material into the bony tunnels and to become fixed. This integration takes a minimum of ten weeks, but the graft itself is not “mature”/strong enough for participating in contact sports for at least six to nine months.
Rehabilitation programme:
Post-operative Rehabilitation Phase:
Goals: *
- Control pain and swelling
- Restore normal range of motion
- Develop muscle strength sufficient for normal gait
- Mentally prepare the patient for surgery
1: First two weeks after surgery
The objective is to
- reduce swelling,
- regain muscle control,
- restore your normal gait as well as the ability to extend and flex your knee.
Your physiotherapist will use lots of ice and compression to reduce your swelling. You will be encouraged to exercise in short, regular bursts – say five to ten minutes every hour.
It is important to be able to fully extend and lock your knee as soon as possible. This action helps the quadriceps muscle above the knee to pump blood away from the knee and reduce swelling.
Exercises include hamstring and calf stretches, static contractions of quadriceps and gentle bending.
2: Two to six weeks after surgery
gain confidence and strengthen the knee whilst restoring full flexion.
Typical exercises will include stair climbing, static cycling, knee bends and lunges.
Weights will be introduced and you may begin to swim.
3: Six to twelve weeks after surgery
You will now be gaining in confidence and fitness and will have a regular programme to improve coordination and balance.
The speed and resistance exercises will be increased; progressive hamstring and quadriceps strengthening will continue.
4: Three to six months after surgery
Now the objective is to maintain motivation, improve aerobic fitness and develop sport specific skills.
Your programme will include progressive running and agility skills and a tailored sports programme. Jumping, running and rotating skills will be introduced
.
- Day 1 – Week 6: Full weight bearing ASAP. Range of motion treatment. Muscle strengthening. Training of the reflexes (proprioception). Closed chain exercises only, ie the foot remains in contact with something (such as the floor), so that there is no hopping, skipping, jumping or running.
- Week 6 – Week 12: Commencement of open chain exercises (where the foot can leave the floor) eg running, but no sport
- Up to 9 months: Intensive focussing on muscle strengthening, proprioception and performance of sport-specific training exercises
- From 9 months: Careful return to competitive sport
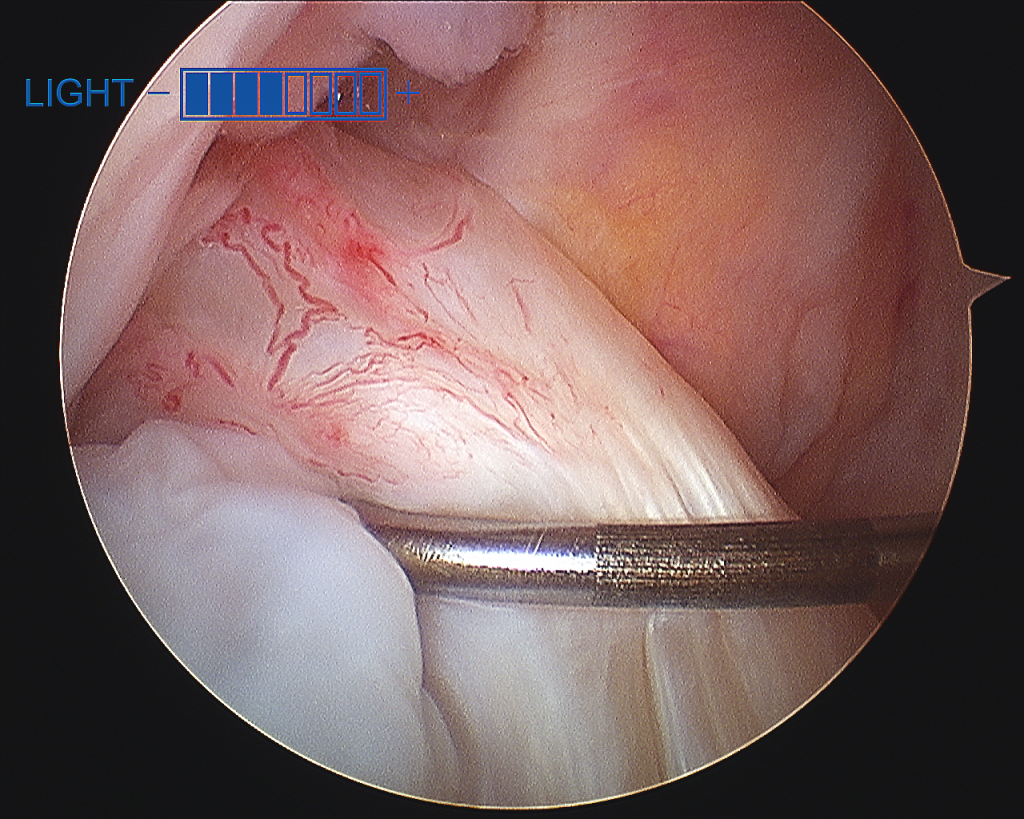
Arthroscopic view of ACL



Types of Grafts

{kind=link}
Sources of autografts.
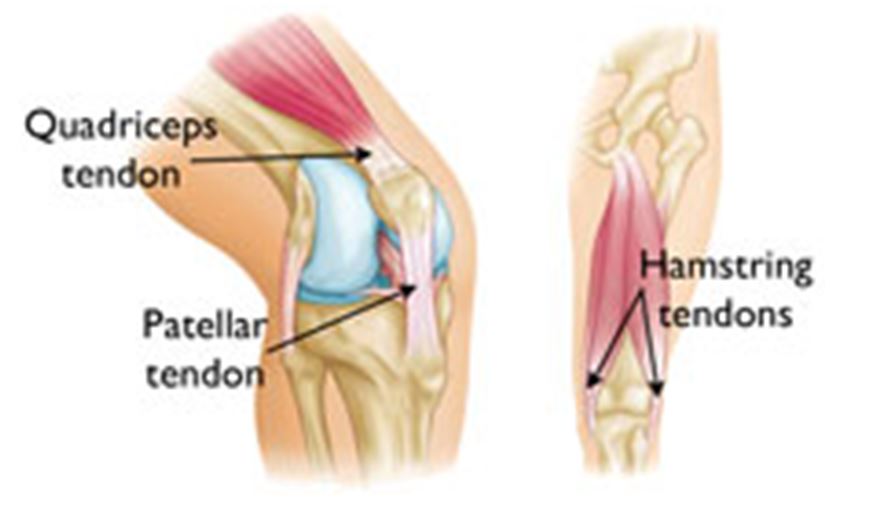
Grafts can be obtained from several sources. Grafts from your own body are called autografts. The most common sources of autografts are:
- The patellar tendon
- The quadriceps tendon
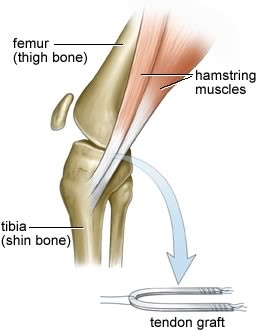
- The hamstring tendons
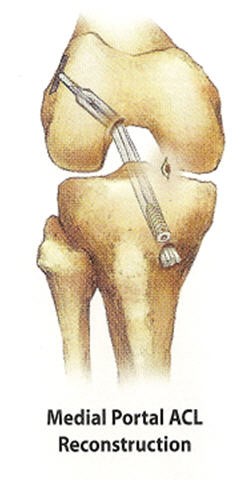
ACL Reconstruction Using Hamstring Autograft





X ray after ACL reconstruction


Post op x ray of ACL surgery